Irritable Bowel Syndrome and Eating Disorders

Understanding overlap, causality, and the traps people fall into
Most people with irritable bowel syndrome (IBS) have tried to fix their symptoms by changing what they eat. Some remove lactose, others gluten, others follow low-FODMAP diets, and many keep narrowing their options over time. What is discussed far less often is why digestion can suddenly feel fragile in the first place, and why food tolerance sometimes returns when sleep, stress, and emotional safety improve.
If food were the root problem for most people with IBS, these patterns would be difficult to explain.
This article explores the scientifically supported overlap between IBS and eating disorders, why food restriction often escalates unintentionally, and how stress and early life experiences can shape digestive vulnerability. Its purpose is not to diagnose or treat eating disorders, but to clarify how these conditions can reinforce each other and how people can become stuck in cycles that feel impossible to escape.
Understanding this interaction is often the first step toward breaking it.
Article in brief
IBS and eating disorders frequently co-occur, and the relationship appears bidirectional rather than one-way (they both affect each other). Food avoidance often accumulates over time, not because people are irrational, but because symptoms are frightening and unpredictable.
Stress and sleep strongly influence symptom severity, while restriction may help short-term but obscure deeper drivers. The most effective long-term outcomes tend to emerge when treatment addresses the whole person, not just food.
Important to know
Eating disorders should never be left untreated. This article is intended to improve understanding of the interaction between IBS and disordered eating patterns, not to diagnose or treat eating disorders. Disordered eating is not the same as an eating disorder: eating out of boredom, eating past fullness, or occasional restriction does not automatically indicate pathology, though they can indicate psychological distress if habitual or if done in response to emotional turmoil or psychological distress.
Eating disorders typically involve persistent fear around food, body-image distress, rigid or compulsive eating behaviors, and patterns that are clearly harmful to physical and psychological health. If you suspect an eating disorder in yourself or someone else, professional medical and psychological support is essential.
The link between IBS and eating disorders
Research consistently shows a strong overlap between irritable bowel syndrome and eating disorders. Globally, IBS affects roughly 10–15% of adults (Ford et al., 2014, Gastroenterology), while eating disorders affect about 9% of the population (Galmiche et al., 2019, The Lancet Psychiatry), though this varies according to study.
Among people diagnosed with eating disorders, 50–90% report functional gastrointestinal symptoms, and 30–50% meet diagnostic criteria for IBS (Hanel et al., 2021, Nutrients).
Studies across clinical and community populations demonstrate that individuals with eating disorder symptoms have a significantly higher likelihood of IBS, and that IBS patients show elevated rates of restrictive or avoidant eating behaviors (Hanel et al., 2021; Spillebout et al., 2019, Reed-Knight et al.,2016). These findings appear across age groups and diagnostic categories.
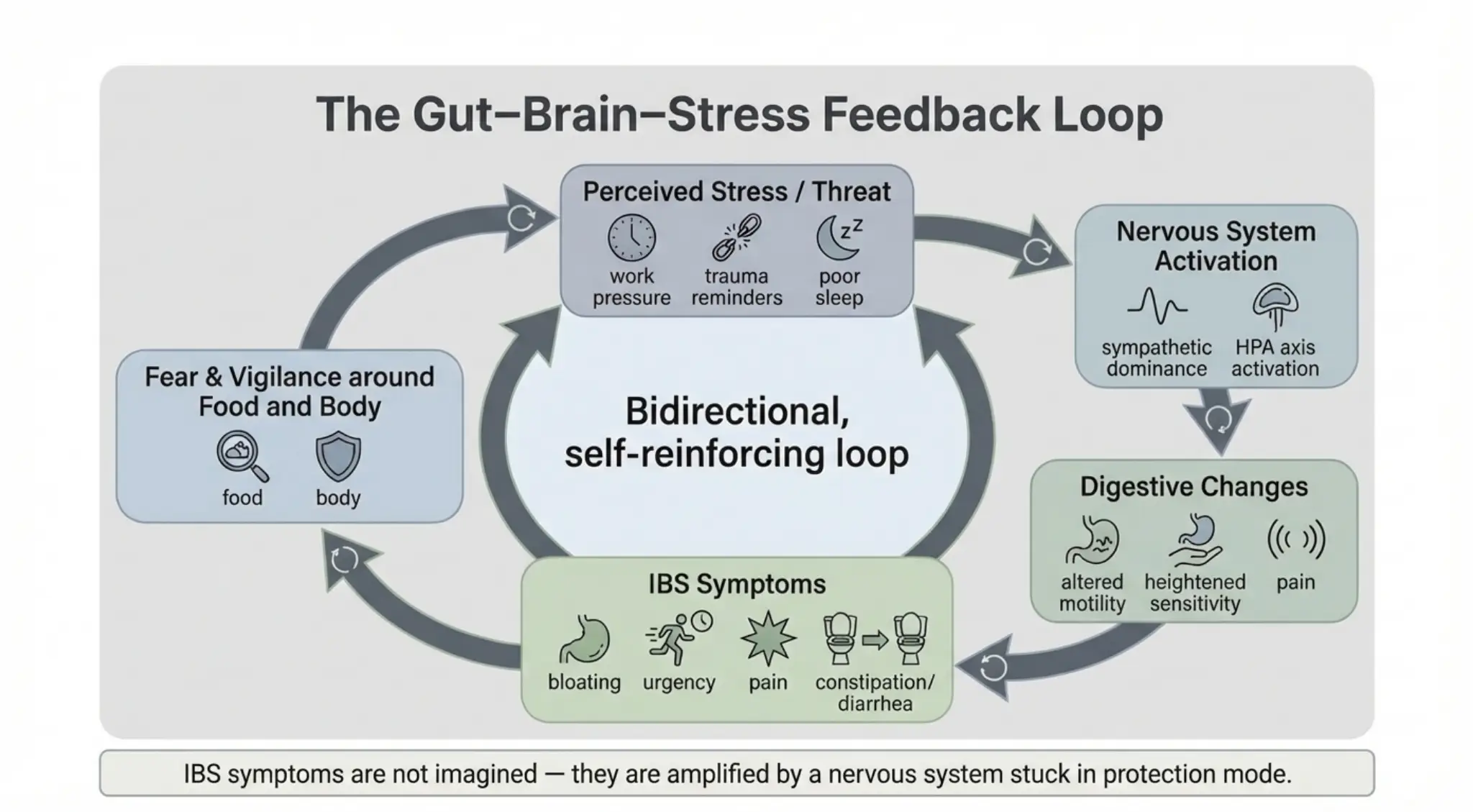
Evidence also clearly shows that psychological distress mediates symptom severity through the gut–brain axis. In other words, when long-term emotional strain is present, the digestive system often becomes more sensitive. Researchers refer to this as the gut–brain axis, the two-way communication pathway linking emotional regulation systems in the brain with digestive function.
Food avoidance as a shared feature
IBS and several eating disorders share a common behavioral pattern: food avoidance. IBS is a functional gastrointestinal disorder, meaning that symptoms arise from altered communication between the nervous system and the gut rather than from structural disease. This altered signaling can affect gut motility (how fast food moves), visceral sensitivity (how strongly sensations are felt), and pain processing.
From a lived perspective, this often means bloating, urgency, constipation, diarrhea, pain, and social withdrawal. Because symptoms frequently appear after eating, many people understandably conclude that food itself must be the problem. Over time, this belief can drive increasing restriction.
Surveys suggest that up to 60% of IBS patients adopt some form of self-directed food avoidance or long-term elimination diet beyond medical advice (Staudacher & Gibson, , 2022 and 2023; Bellini, M., Rossi, A. Is a low FODMAP diet dangerous?, 2018).
Are foods themselves the real problem?
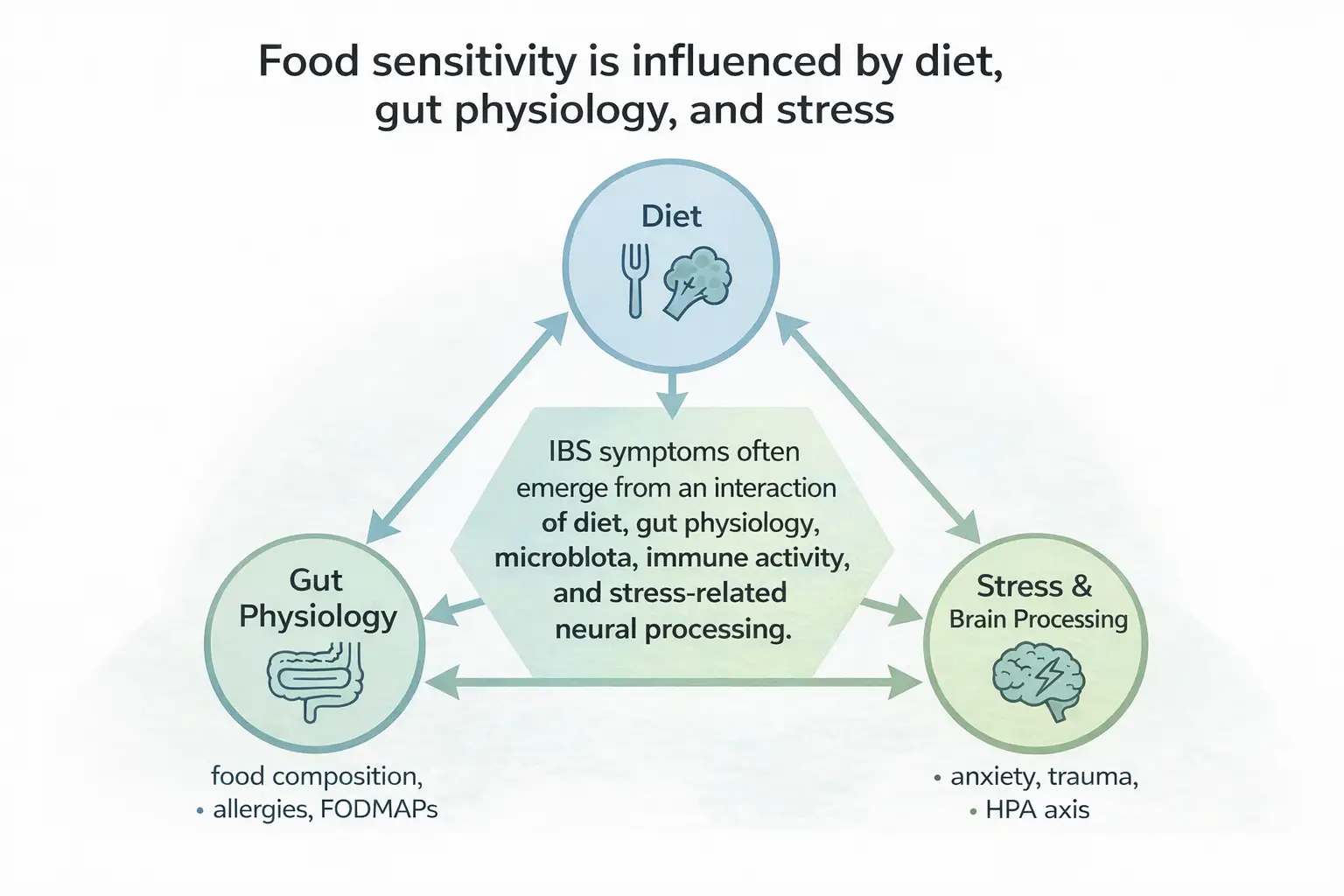
Food can clearly provoke symptoms in IBS through fermentation, osmotic effects, or mechanical load, and dietary therapy such as the low-FODMAP diet remains one of the most evidence-based short-term interventions for symptom reduction. However, food is rarely the sole underlying cause of IBS. Instead, it acts as a modulator within a system already rendered sensitive by multiple interacting biological and environmental factors, including microbiota changes and physiological stress responses (Ng et al., 2023). Therefore, psychological wellbeing and proper sleep are extremely important.
Therefore, when discussing long-term treatment, it is important to take into account long-term techniques for relief as well. Notably, both sleep disturbances and psychological distress alter gut motility, visceral sensitivity, immune signaling, and pain processing.
In other words, when stress stays switched on (either due to bad sleep or psychological stress), it doesn’t just affect mood. It changes the rhythm of digestion, how strongly the gut reacts to normal sensations, and how the immune system interprets safety signals. This is the physiology beneath what many people experience simply as “tension in the stomach.”
Stress as a central amplifier:
Why your gut reacts when life does
Stress is not merely a trigger for IBS symptoms; it is a central amplifier. Many people report the onset of IBS following periods of sustained stress, illness, or life disruption. Research shows that early-life adversity, including childhood trauma, significantly increases the risk of developing IBS in adulthood (Park et al., 2016).
Meta-analyses indicate that individuals exposed to childhood abuse or neglect have approximately two- to threefold higher odds of developing IBS and other somatic syndromes as adults compared with those without such histories (Afari et al., 2014; AJHB, 2025).
A key biological pathway involved is the HPA axis, the hypothalamic–pituitary–adrenal system, that regulates the body’s stress response and cortisol release. When this system remains chronically activated, digestive sensitivity increases and tolerance decreases.
Dietary restriction: relief and risk
Restricting food intake can temporarily reduce symptoms by lowering digestive workload, which is why elimination diets can be clinically useful when applied correctly. Problems arise when restriction becomes long-term and disconnected from reintroduction, nervous-system regulation, or psychological support.
Over time, chronic restriction, even through FODMAP-diets, can reduce microbiota diversity, increase anxiety around eating, and begin to resemble eating-disorder behaviors, even in people who never intended to develop them (Staudacher & Whelan, 2016, 2017).
Which comes first: IBS or eating disorders?
The relationship between IBS and eating disorders appears bidirectional. Longitudinal data suggest that disordered eating behaviors in adolescence increase the risk of IBS in adulthood (Yang et al., 2024). Conversely, IBS patients show higher rates of restrictive eating patterns, including avoidant or restrictive presentations (Murray & Staller, 2021).
Some studies indicate that eating disorders more often precede IBS, while others show the reverse in a minority of cases (Perkins et al., 2005; Almeida et al., 2024). Clinically, what matters is not which came first, but how each condition reinforces the other once both are present.
Regulation before expansion
Across both research and clinical experience, symptom improvement often parallels reductions in chronic stress and improvements in sleep. As nervous-system regulation improves, digestive tolerance frequently increases. Foods once considered “unsafe” may become tolerable again, although individual limits can remain (Mulianda et al., 2023).
Psychological interventions that target stress processing, including cognitive-behavioral therapy and gut-directed hypnotherapy, reduce overall IBS symptom severity by an average of 48–60%, with benefits often sustained for 6–12 months post-treatment (Ford et al., 2014, American Journal of Gastroenterology) .
Therapeutic approaches in context
In my coaching practice, I draw on schema-informed approaches and EFT techniques alongside lifestyle and regulation work to help clients reduce chronic stress and restore a sense of safety in the body. These methods align with the gut–brain mechanisms identified in the research, particularly those involving threat perception, emotional processing, and autonomic regulation.
Early evidence also supports stress-regulation techniques similar to those used in coaching and energy psychology frameworks. For example, Emotional Freedom Techniques (EFT) have shown moderate-to-large effect sizes (Cohen’s d = 0.6–0.8) for reducing physiological stress markers and anxiety symptoms (Church et al., 2018), aligning with gut–brain models that link safety perception to digestive function.
What science shows and what it often means in practice
| What research shows | What this often means for people |
|---|---|
| IBS is stress-responsive | Symptoms worsen during emotional overload, not just after meals |
| Food triggers are context-dependent | Tolerance varies with sleep, safety, and stress |
| Restriction reduces symptoms short-term | Relief can mask deeper vulnerability |
| Nervous-system regulation improves outcomes | Healing often feels indirect and slower than diet changes |
If this article resonated with you, you can reach out here:
Tell me a little about your situation, and we’ll see how we can make you feel better. Together.
References
- https://onlinelibrary.wiley.com/doi/10.1002/erv.2847
- https://www.thelancet.com/journals/langas/article/PIIS2468-1253(20)30217-X/abstract
- https://www.mdpi.com/2072-6643/15/11/2501
- https://www.sciencedirect.com/science/article/pii/S039876201930433X?via%3Dihub
- https://onlinelibrary.wiley.com/doi/10.1111/nmo.12894
- https://onlinelibrary.wiley.com/doi/10.1111/apt.18197
- https://link.springer.com/article/10.1007/s10151-018-1835-9
- https://www.cghjournal.org/article/S1542-3565(22)00608-5/fulltext
- https://www.cghjournal.org/article/S1542-3565(21)01031-4/fulltext
- https://www.mdpi.com/2218-1989/13/4/484
- https://www.sciencedirect.com/science/article/abs/pii/S0022399917309194?via%3Dihub
- https://onlinelibrary.wiley.com/doi/10.1111/nmo.12826
- https://journals.lww.com/bsam/abstract/2014/01000/psychological_trauma_and_functional_somatic.2.aspx
- https://onlinelibrary.wiley.com/doi/10.1002/ajhb.24209
- https://www.frontiersin.org/journals/pediatrics/articles/10.3389/fped.2023.1241801/full
- https://www.sciencedirect.com/science/article/pii/S2352289521000564?via%3Dihub
- https://www.cambridge.org/core/journals/proceedings-of-the-nutrition-society/article/altered-gastrointestinal-microbiota-in-irritable-bowel-syndrome-and-its-modification-by-diet-probiotics-prebiotics-and-the-low-fodmap-diet/8A7E00D44BD17B2F192D8EEBE464AD03
- https://gut.bmj.com/content/66/8/1517
- https://onlinelibrary.wiley.com/doi/10.1111/apt.18197
- https://onlinelibrary.wiley.com/doi/10.1002/erv.2847
- https://www.sciencedirect.com/science/article/abs/pii/S0022399904005446?via%3Dihub
- https://onlinelibrary.wiley.com/doi/10.1111/nmo.14782
- https://www.jepublichealth.com/index.php/jepublichealth/article/view/565
- https://journals.lww.com/ajg/abstract/2014/09000/effect_of_antidepressants_and_psychological.10.aspx
- https://www.mdpi.com/2227-9032/6/4/146
- https://onlinelibrary.wiley.com/doi/10.1002/smi.3226
- https://www.frontiersin.org/journals/psychology/articles/10.3389/fpsyg.2024.1293150/full