Irritable Bowel Syndrome and Eating Disorders

Understanding the overlap, the traps, and why food is rarely the whole story
Eating disorders are surprisingly common, especially among women. IBS shows a similar pattern, though of course men are affected too. Since both conditions significantly reduce quality of life and affect sufferers on a near-daily basis, it’s worth taking a serious look at how IBS and eating disorders are connected, how they interact, and what that means for anyone caught between the two.1, 2, 3
I’ve been working with IBS clients since 2021, and I went through my own period of debilitating IBS as well as a mild eating disorder. So, in this article I’ll go through some questions I think are worth asking: can IBS cause eating disorders, can eating disorders cause IBS, what do these conditions share, and how can people actually start to move forward? (NOTE: if you are suffering from an eating disorder, please contact a licensed specialist.)
Article in brief
IBS and eating disorders occur together relatively often and seem to influence one another in both directions. Food avoidance tends to build up over time, because IBS symptoms are frightening and unpredictable, and cutting out food feels very logical. Stress, especially emotional stress, and poor sleep are also strongly tied to an increased risk of IBS and to worse symptoms. The most meaningful improvements often come when treatment addresses the whole person, not just the diet.4, 5, 6, 7
Important to know
An eating disorder should never be left untreated. This article is intended to help you understand the connection between IBS and eating disorders, and it cannot be used to diagnose or treat either condition.
It’s also worth noting that disordered eating is not the same thing as an eating disorder. Skipping meals, limiting foods, or following restrictive diets can all count as disordered eating patterns, especially when they become regular. But the line between “this is how I manage symptoms” and “this has become a clinical problem” depends on severity, motivation, and consequences: weight loss, inadequate nutrition, fear, social impairment, or a life that starts revolving around food avoidance.5
A clinical eating disorder usually involves long-term fear around food, distressing thoughts about your body and self-worth, compulsive eating behaviours, and patterns that are clearly harmful to physical and psychological health. If you suspect that you or someone you know is dealing with an eating disorder, please see a doctor.
The connection between IBS and eating disorders
The overlap between IBS and eating disorders is bigger than most people expect. IBS prevalence depends heavily on diagnostic criteria: one global meta-analysis found a pooled prevalence of 9.2% using Rome III criteria, but 3.8% using the stricter Rome IV criteria. Eating-disorder estimates also vary quite a bit, but one systematic review found lifetime eating-disorder prevalence of 8.4% in women and 2.2% in men, while more recent point-prevalence estimates rose to 7.8% in the 2013–2018 period. So yes, eating disorders are common enough that this is not some tiny side issue.1, 3
And when we look specifically at people with eating disorders, gut symptoms are everywhere. In one female inpatient eating-disorder sample, 98% met criteria for at least one functional gastrointestinal disorder and 52% met criteria for IBS. Another study found that 64% of people with a current or past eating disorder met Manning criteria for IBS. Across both clinical and community samples, people with eating-disorder symptoms are more likely to also have IBS, and IBS patients show higher rates of restrictive or avoidant eating than people without IBS.8, 10, 4, 11, 5, 12
The connection between the two runs mostly through what researchers call the gut-brain axis, which is the two-way communication system between the digestive tract and the central nervous system. When someone is under chronic emotional stress, the digestive system can become more sensitive and reactive. This isn’t a loose metaphor, mind you (pun not intended, but probably understood by those of us who have diarrhoea-based IBS). Psychological stress can affect gut motility, visceral sensitivity (how your intestines feel stuff), secretion, permeability (how easily things from your gut can pass through the intestinal wall into your bloodstream), immune activation, the microbiota, and pain processing. In other words, “nervous stomach” is an annoyingly accurate phrase.6, 13
The obvious next question is which comes first, and the honest answer is that we don’t fully know. It probably varies between people. What the evidence does suggest is that the relationship runs in both directions. Issues with excessive weight-control and negative eating behaviours in teenage years seem to increase IBS risk in adulthood. In one eating-disorder sample, 87% had developed the eating disorder before IBS symptoms started. Another study found that most patients had an eating-disorder diagnosis before their gastrointestinal consultation, though that tells us about clinical timing, not necessarily the exact biological starting point. Then again, IBS can clearly push people into food avoidance, restriction, and fear-based eating.31, 10, 32, 5, 19
There is also something called avoidant/restrictive food intake disorder, or ARFID, which basically means someone restricts food so much that it affects their health, nutrition, weight, or life. And, yes, in many cases this sounds very much like what happens with severe cases of IBS. One adult outpatient gastrointestinal clinic study found that 19% of patients screened positive for ARFID, and IBS patients were twice as likely as non-IBS patients to screen positive. So when someone is afraid to eat, avoids more and more foods, loses weight, needs supplements, or stops eating socially, we should not shrug and call it “just IBS.” That would be dismissive and demeaning. Sadly, this does happen more often than it ever should.5, 19
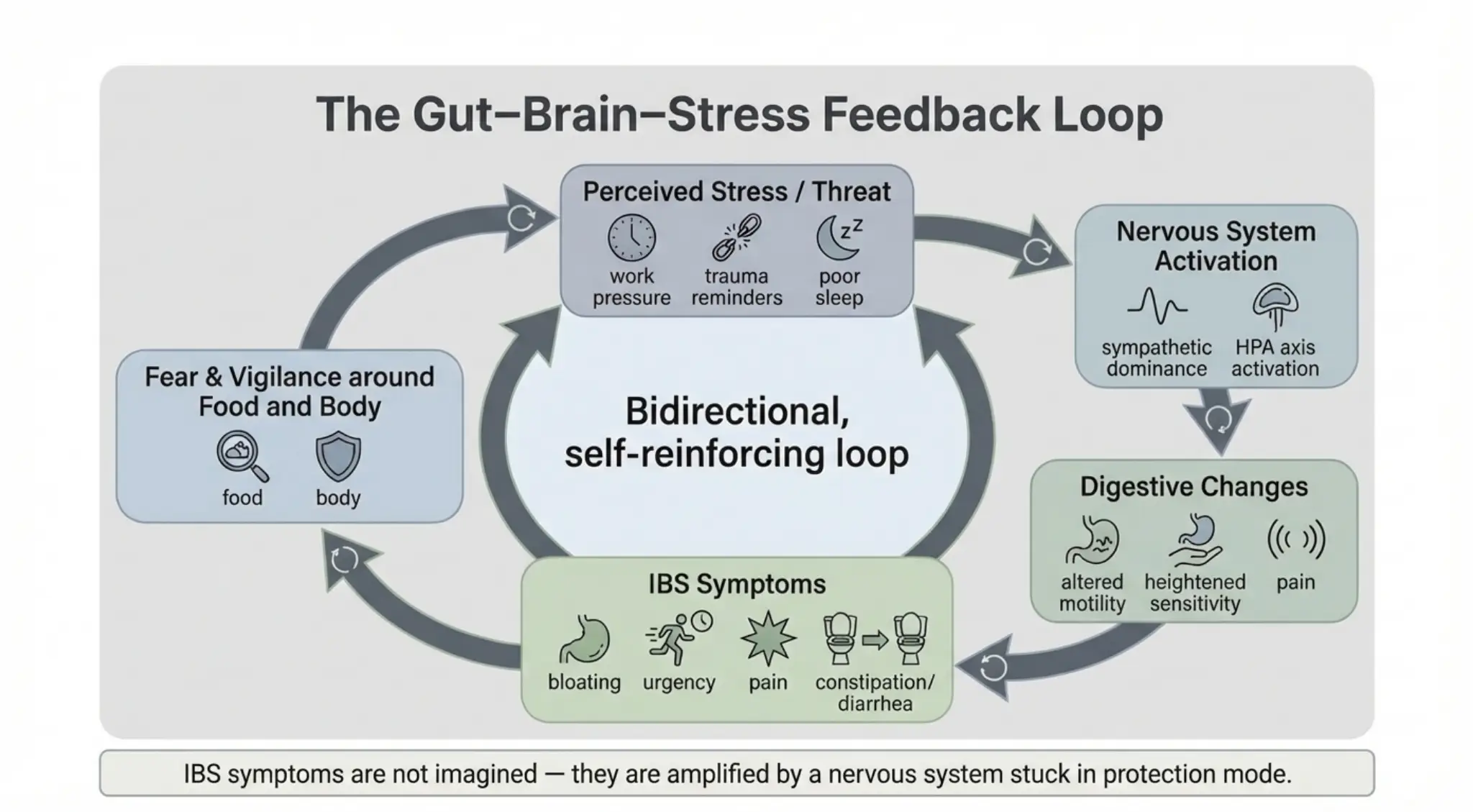
However, if we’re brutally practical, the question of which comes first isn’t always all that important, because once both are present, they create an effective loop: symptoms increase restriction, restriction increases anxiety, anxiety increases symptoms… in the end you feel you need to restrict more and more just to survive.
Food avoidance: completely understandable, increasingly dangerous
When you understand what IBS actually feels like (severe bloating, urgent and unpredictable trips to the toilet, constipation, diarrhoea, pain, gas that could clear a room), it makes complete sense that people start connecting symptoms to food. Eating is often the most recent thing that happened before the symptoms hit, so the brain draws the obvious conclusion.
So people start eliminating. First the obvious suspects, then a few more, then a few more after those. This gets even worse once you do a bit of Googling and find the FODMAP diet (raise hands if you’ve done a bit of Googling, or “AI:ing”, for a problem you have. Yeah, same here). Once you do, “all carbs are bad” becomes a very easy, though wrong and extreme, conclusion.
According to research, more than 60% of IBS patients have already independently limited or excluded foods before seeing a gastroenterologist.15 Sadly, restrictive diets can become stressful, socially limiting, and hard to step back from once the brain has learned “food equals danger”. The low-FODMAP diet is one of the better-supported short-term dietary interventions for IBS, but it is meant to be structured, temporary, and followed by reintroduction and personalisation. Not a “goodbye carbs, spices, and everything I love” forever.16, 17, 5
You see, long-term restriction doesn’t just affect calories. It can reduce food variety, lower nutrient intake, make social eating harder, and in some people start looking a lot like clinically problematic avoidant or restrictive eating. Low-FODMAP restriction can also change the gut microbiota, including reductions in Bifidobacteria, though the long-term meaning of those changes is still not fully clear. And, ironically enough, the fear and stress around eating can themselves feed (hah! Sorry, couldn’t resist) IBS symptoms, which then seem to confirm that the restriction was the right call.18, 16, 5, 19, 6, 20
At its worst, you end up in a situation where you either eat too little and avoid the horrible symptoms, or you eat normally and suffer. Most people eventually find some kind of a balance, but in some cases there isn’t any clear food to restrict at all. This is what happened to me, when my doctors told me to “avoid foods that annoy your stomach.” All foods annoyed me. In cases like that, people tend to either panic their way into eating almost nothing, or think “sod it all” and just eat in pain. Neither is a liveable balance, nor does it have to be the permanent state of affairs.
So is food actually the problem?
Food can genuinely provoke IBS symptoms and dietary changes can provide real relief, especially in the short term. So no, this is not me saying “just relax and eat beans”. That would be both unhelpful and, depending on the room, socially catastrophic. I get to make this joke because, at my worst, people around me quite literally did not want to be around me.
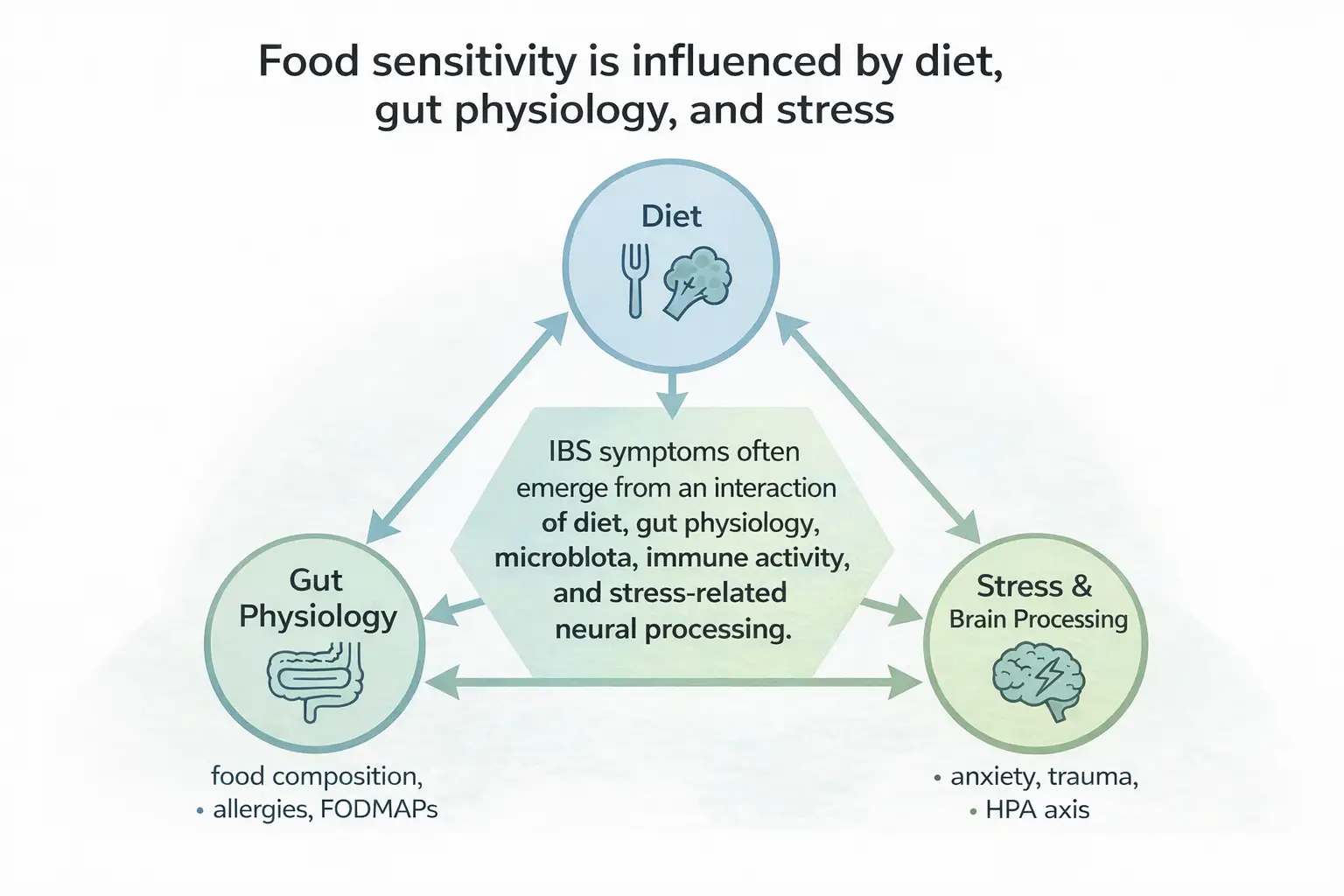
But IBS is rarely just a food problem. It is better understood as a brain-gut-microbiome problem, and diet is only one part of what drives it.16, 6, 13, 14
In normal human language: the same meal can feel completely fine on Tuesday and absolutely devastating on Thursday, because your gut isn’t just reacting to the food. It is also reacting to your sleep, mental state, tiredness, stress load, fear, and so many other things.7, 6, 13
And stress doesn’t just trigger symptoms in people who already have IBS. For many people it seems to have been there at the beginning. Almost every client I’ve worked with can trace the start of their IBS to a period of sustained stress, a major life change, an illness, or a difficult childhood. Research supports this general pattern: adverse childhood experiences and childhood trauma are linked with higher odds of IBS in adulthood, though the exact size of the effect varies between studies.22, 23, 24, 6
This is also why focusing exclusively on what you eat will always leave a significant part of the problem unaddressed when it comes to long-term improvement.
The physiological reason for this runs partly through the HPA axis (the hypothalamic-pituitary-adrenal system – dunno if that actually helped you, but you’re welcome), which regulates the body’s stress response and cortisol production. When this system has been repeatedly activated, especially early in life, the body can become more reactive to threat later on. In less academic terms: the nervous system gets jumpy, and the gut joins the committee.6, 25, 26
The cultural side of food fear
It’s also worth talking about something that rarely gets discussed in IBS circles: the cultural and social environment that shapes how people, especially young women, relate to food and their bodies in the first place. I strongly feel that eating disorders are very much a by-product of a mixture of things working together; teasing, thoughtless comments from adults, fashion magazines, social media, and the toys we hand children as supposed models of the human form. There is also some science to back this up, such as research linking bullying and teasing with eating disorders, experimental work showing that exposure to Barbie images can affect body esteem in young girls, and broader evidence that exposure to idealised body images and social comparison can worsen body image and eating-disorder symptoms.27, 28, 29, 30
The obvious examples are everywhere: body ideals in media, casual comments from adults, school teasing, family food rules, and the general weirdness of growing up in a world where children are somehow expected to develop a healthy relationship with food while constantly being told which bodies are acceptable. And yes, some toys and action figures look less like humans and more like someone lost a fight with Photoshop and testosterone.
These are the templates children absorb, often without anyone around them naming what’s actually happening.
This matters for IBS because parents who struggle with eating disorders, disordered eating, body shame, or fear around food can, through their own behaviour and language around food, pass some of those patterns on to children, often unintentionally. And those patterns, combined with a nervous system already affected by stress, shame, or negative experiences around school, can make eating feel scary. That does not mean parents are to blame, but children learn from the emotional weather around them, including the weather around food, bodies, stress, and control. Prevention, then, has to happen at a social level too: schools teaching emotion regulation and empathy, families having honest conversations about body image, and society at large becoming a little more sceptical of the idea that a very narrow range of body shapes constitutes health or worth.5, 27, 6, 22
What actually produces lasting improvement
Across both the research and my own practice, the pattern is fairly consistent: when stress regulation, sleep, emotional processing, and the relationship with food improve, digestive tolerance often improves alongside them. Not always completely, and not always evenly, since some individual sensitivities do remain. But the overall direction is toward a more functional and less frightening relationship with food and the body.6, 20, 33, 5
Psychological therapies also have evidence for IBS. Cognitive behavioural therapy, hypnotherapy, multicomponent psychological therapy, and dynamic psychotherapy have all shown benefit compared with control therapy or usual management. Of course that doesn’t mean that talking about it a few times creates magical changes. What it does mean, though, is that working with the brain, and the nervous system as a whole, can be a truly meaningful addition to the treatment plan.34, 33, 20
In my own work, I draw on schema-informed approaches (essentially dealing with childhood issues through visualisations), EFT (Emotional Freedom Techniques), sleep work, and lifestyle changes. I use those because they target the stress, safety, and emotional-processing patterns that often are at the root of the symptoms. We also know from studies that anxiety, depressive moods, and stress generally speaking affect IBS very strongly, which is why I find a combination of schema-informed approaches and EFT very useful in practice.7, 6, 20, 35
None of this means diet doesn’t matter, because it does, but it works best as one part of a broader picture rather than the whole answer.
How to actually move forward with food
If restriction has become a significant part of the picture, expanding the diet is something that needs to happen, carefully and gradually. The general principle is the same as elimination but in reverse: one food at a time, starting with small amounts, and giving it enough time to get a clear read. For vegetables in particular, well-cooked is usually better tolerated than raw, so starting there and slowly reducing the cooking time as tolerance improves is a sensible approach. Though as a general point, please don’t attempt to eat raw potatoes. That’s a separate problem entirely, and not a fun one.
If there’s an active eating disorder alongside the IBS, or if someone is losing weight, panicking around food, needing supplements, avoiding social eating, or living on a tiny list of “safe” foods, the reintroduction process should happen with a registered dietitian rather than alone and preferably alongside the help of a licensed therapist who specialises in eating disorders.5, 19, 15
And if a reintroduction goes badly, that’s not a verdict on the food. Give it another go when life is a bit easier.5, 19, 15
What clients say
Below are three clients I’ve worked with. While their symptoms were different, they all had experienced daily food restriction and everyone’s symptoms improved when lifehabit coaching was combined with psychological work.
Maria — 8 sessions over 4 months
“My gut was really sensitive at first and reacted strongly to changes. Now, it’s almost back to normal, and I can eat foods I couldn’t before. Working with Kevin has been a breeze. He’s easy to talk to, and we’ve had plenty of laughs. I’ve gained a lot of insight into my mindset and behaviour, especially as we’ve worked through my childhood traumas.”
Tanja — 8 sessions over 4 months
“My sleep has improved tremendously and my IBS is remarkably calm. Kevin knows how to make clients feel safe even when dealing with extremely difficult topics, which is key when working with trauma.”
Ville — 5 sessions over 6 months
“The biggest thing I’ve learned with Kevin is how to manage stress. He also gave great advice on supplements and eating. Now if I eat something my stomach doesn’t like, it is fine in just a day. Before it took up to even 4 days to calm down. I really like how Kevin’s coaching isn’t all super serious, even though it’s definitely professional.”
You can read these and more testimonials here.
In summary
| What research shows | What this often means for people |
|---|---|
| IBS is stress-responsive | Symptoms often worsen during emotional overload, not just after meals |
| Food triggers are context-dependent | Tolerance shifts with sleep, stress, and how safe the nervous system feels |
| Restriction reduces symptoms short-term | The relief can mask deeper sensitivity rather than resolve it |
| Brain-gut and psychological interventions can help | Improvements often come from reducing threat, fear, stress, and symptom reactivity, not only from changing food |
| IBS and eating disorders both influence each other | Each condition can drive the other, creating cycles that are hard to exit without addressing both |
| Early adversity is linked with higher odds of IBS in adulthood | For many people, gut sensitivity has roots that predate any particular food |
If this resonated and you’d like to talk about your situation:
As someone who went from suicidal thoughts due to my IBS to living almost entirely symptom free, I want to help you achieve that too.
References and further reading
- Oka, P., Parr, H., Barberio, B., Black, C. J., Savarino, E. V., & Ford, A. C. (2020). Global prevalence of irritable bowel syndrome according to Rome III or IV criteria: a systematic review and meta-analysis. The Lancet Gastroenterology & Hepatology. SourceReferenced above: 1, 2
- Kim, Y. S., & Kim, N. (2018). Sex-Gender Differences in Irritable Bowel Syndrome. Journal of Neurogastroenterology and Motility, 24(4), 544–558. SourceReferenced above: 1
- Galmiche, M., Déchelotte, P., Lambert, G., & Tavolacci, M. P. (2019). Prevalence of eating disorders over the 2000–2018 period: a systematic literature review. The American Journal of Clinical Nutrition, 109(5), 1402–1413. SourceReferenced above: 1, 2
- Hanel, V., Schalla, M. A., & Stengel, A. (2021). Irritable bowel syndrome and functional dyspepsia in patients with eating disorders: a systematic review. European Eating Disorders Review. SourceReferenced above: 1, 2, 3
- Harer, K. N. (2019). Irritable Bowel Syndrome, Disordered Eating, and Eating Disorders. Gastroenterology & Hepatology, 15(5), 280–282. SourceReferenced above: 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12
- Qin, H.-Y., Cheng, C.-W., Tang, X.-D., & Bian, Z.-X. (2014). Impact of psychological stress on irritable bowel syndrome. World Journal of Gastroenterology, 20(39), 14126–14131. SourceReferenced above: 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14
- Mulianda, C. A., Murti, B., & Prasetya, H. (2023). Associations between Anxiety, Depression, and Poor Quality of Sleep on the Risk of Irritable Bowel Syndrome: A Meta-Analysis. Journal of Epidemiology and Public Health. SourceReferenced above: 1, 2, 3
- Boyd, C., Abraham, S., & Kellow, J. (2005). Psychological features are important predictors of functional gastrointestinal disorders in patients with eating disorders. Scandinavian Journal of Gastroenterology, 40(8), 929–935. SourceReferenced above: 1, 2
- Carpinelli, L., Savarese, G., Pascale, B., Milano, W. D., & Iovino, P. (2023). Gut–Brain Interaction Disorders and Anorexia Nervosa: Psychopathological Asset, Disgust, and Gastrointestinal Symptoms. Nutrients. SourceReferenced above: 1
- Perkins, S. J., Keville, S., Schmidt, U., & Chalder, T. (2005). Eating disorders and irritable bowel syndrome: is there a link? Journal of Psychosomatic Research, 59(2), 57–64. SourceReferenced above: 1, 2
- Spillebout, A., Déchelotte, P., Ladner, J., & Tavolacci, M. P. (2019). Mental health among university students with eating disorders and irritable bowel syndrome in France. Revue d’Épidémiologie et de Santé Publique. SourceReferenced above: 1, 2
- Reed-Knight, B., Squires, M., Chitkara, D. K., & van Tilburg, M. A. L. (2016). Adolescents with irritable bowel syndrome report increased eating-associated symptoms, changes in dietary composition, and altered eating behaviors. Neurogastroenterology & Motility. SourceReferenced above: 1
- Padhy, S. K., Sahoo, S., Mahajan, S., & Sinha, S. K. (2015). Irritable bowel syndrome: Is it “irritable brain” or “irritable bowel”? Journal of Neurosciences in Rural Practice, 6(4), 568–577. SourceReferenced above: 1, 2, 3, 4, 5
- Ng, Q. X., Yau, C. E., Yaow, C. Y. L., Chong, R. I. H., Chong, N. Z.-Y., Teoh, S. E., Lim, Y. L., Soh, A. Y. S., Ng, W. K., & Thumboo, J. (2023). What Has Longitudinal ‘Omics’ Studies Taught Us about Irritable Bowel Syndrome? A Systematic Review. Metabolites. SourceReferenced above: 1
- Bellini, M., & Rossi, A. (2018). Is a low FODMAP diet dangerous? Techniques in Coloproctology. SourceReferenced above: 1, 2, 3, 4
- Staudacher, H. M., & Whelan, K. (2017). The low FODMAP diet: recent advances in understanding its mechanisms and efficacy in IBS. Gut. SourceReferenced above: 1, 2, 3
- Staudacher, H. M., & Gibson, P. R. (2023). Traditional Dietary Advice, Low FODMAP Diet, or Gluten-Free Diet for IBS: Growing Understanding but Uncertainties Remain. Clinical Gastroenterology and Hepatology. SourceReferenced above: 1
- Staudacher, H. M., & Whelan, K. (2016). Altered gastrointestinal microbiota in irritable bowel syndrome and its modification by diet: probiotics, prebiotics and the low FODMAP diet. Proceedings of the Nutrition Society. SourceReferenced above: 1
- Burton Murray, H., & Staller, K. (2022). When Food Moves From Friend to Foe: Why Avoidant/Restrictive Food Intake Matters in Irritable Bowel Syndrome. Clinical Gastroenterology and Hepatology. SourceReferenced above: 1, 2, 3, 4, 5, 6
- Sibelli, A., Chalder, T., Everitt, H., Chilcot, J., & Moss-Morris, R. (2018). Positive and negative affect mediate the bidirectional relationship between emotional processing and symptom severity and impact in irritable bowel syndrome. Journal of Psychosomatic Research. SourceReferenced above: 1, 2, 3, 4
- Horn, A., Stangl, S., Parisi, S., Bauer, N., Roll, J., Löffler, C., Gágyor, I., Haas, K., Heuschmann, P. U., Langhorst, J., & Keil, T. (2023). Systematic review with meta-analysis: Stress-management interventions for patients with irritable bowel syndrome. Stress and Health. SourceReferenced above: 1, 2
- Park, S. H., Videlock, E. J., Shih, W., Presson, A. P., Mayer, E. A., & Chang, L. (2016). Adverse childhood experiences are associated with irritable bowel syndrome and gastrointestinal symptom severity. Neurogastroenterology & Motility. SourceReferenced above: 1, 2, 3, 4
- Lenover Moyer, M. B., Jasani, K., Waldman, A. B., Chinchilli, V. M., & Shenk, M. K. (2025). The Developmental Origins of Irritable Bowel Syndrome: A Systematic Review and Meta-Analysis. American Journal of Human Biology. SourceReferenced above: 1, 2, 3
- Afari, N., Ahumada, S. M., Wright, L. J., Mostoufi, S., Golnari, G., Reis, V., & Cuneo, J. G. (2014). Psychological Trauma and Functional Somatic Syndromes: A Systematic Review and Meta-Analysis. Psychosomatic Medicine. SourceReferenced above: 1, 2
- Zhou, G. Q., Huang, M. J., Yu, X., Zhang, N. N., Tao, S., & Zhang, M. (2023). Early life adverse exposures in irritable bowel syndrome: new insights and opportunities. Frontiers in Pediatrics. SourceReferenced above: 1, 2
- Coley, E. J. L., Mayer, E. A., Osadchiy, V., Chen, Z., Subramanyam, V., Zhang, Y., Hsiao, E. Y., Gao, K., Bhatt, R., Dong, T., Vora, P., Naliboff, B., Jacobs, J. P., & Gupta, A. (2021). Early life adversity predicts brain-gut alterations associated with increased stress and mood. Neurobiology of Stress. SourceReferenced above: 1
- Lie, S. Ø., Rø, Ø., & Bang, L. (2019). Is bullying and teasing associated with eating disorders? A systematic review and meta-analysis. International Journal of Eating Disorders, 52(5), 497–514. SourceReferenced above: 1, 2, 3
- Dittmar, H., Halliwell, E., & Ive, S. (2006). Does Barbie make girls want to be thin? The effect of experimental exposure to images of dolls on the body image of 5- to 8-year-old girls. Developmental Psychology, 42(2), 283–292. SourceReferenced above: 1, 2
- Hausenblas, H. A., Campbell, A., Menzel, J. E., Doughty, J., Levine, M., & Thompson, J. K. (2013). Media effects of experimental presentation of the ideal physique on eating disorder symptoms: A meta-analysis of laboratory studies. Clinical Psychology Review, 33(1), 168–181. SourceReferenced above: 1, 2
- Bonfanti, R. C., Melchiori, F., Teti, A., Albano, G., Raffard, S., Rodgers, R., & Lo Coco, G. (2025). The association between social comparison in social media, body image concerns and eating disorder symptoms: A systematic review and meta-analysis. Body Image, 52, 101841. SourceReferenced above: 1, 2
- Yang, K., Kwon, S., Burton-Murray, H., Kuo, B., Chan, A. T., Field, A. E., & Staller, K. (2024). Maladaptive weight control and eating behaviours in female adolescents/young adults are associated with increased risk of irritable bowel syndrome in adulthood: Results from the Growing Up Today Study. Alimentary Pharmacology & Therapeutics. SourceReferenced above: 1
- Almeida, M. N., Atkins, M., Garcia-Fischer, I., Weeks, I. E., Silvernale, C. J., Samad, A., Rao, F., Burton-Murray, H., & Staller, K. (2024). Gastrointestinal diagnoses in patients with eating disorders: A retrospective cohort study 2010–2020. Neurogastroenterology & Motility. SourceReferenced above: 1
- Shafiei, F., Dehghani, M., Fathali Lavasani, F., Manouchehri, M., & Mokhtare, M. (2024). Intensive short-term dynamic psychotherapy for irritable bowel syndrome: a randomized controlled trial examining improvements in emotion regulation, defense mechanisms, quality of life, and IBS symptoms. Frontiers in Psychology. SourceReferenced above: 1, 2, 3
- Ford, A. C., Quigley, E. M. M., Lacy, B. E., Lembo, A. J., Saito, Y. A., Schiller, L. R., Soffer, E. E., Spiegel, B. M. R., & Moayyedi, P. (2014). Effect of Antidepressants and Psychological Therapies, Including Hypnotherapy, in Irritable Bowel Syndrome: Systematic Review and Meta-Analysis. American Journal of Gastroenterology. SourceReferenced above: 1, 2
- Church, D., Stapleton, P., Mollon, P., Feinstein, D., Boath, E., Mackay, D., & Sims, R. (2018). Guidelines for the Treatment of PTSD Using Clinical EFT (Emotional Freedom Techniques). Healthcare. SourceReferenced above: 1